
14 Nov Knee Injections & Viscosupplementation in Singapore: An Evidence‑Based 2025 Guide by Dr Gerard Ee
Reviewed by Dr Gerard Ee — a Singapore physician with a special interest in orthopaedics and knee pain, and co‑author of peer‑reviewed knee surgery research including work in The Knee on computer‑navigation for joint‑line measurement in total knee arthroplasty.
Knee injections are a non‑surgical way to reduce pain and improve function when osteoarthritis or overuse has made daily life difficult. The main options in Singapore are hyaluronic acid (HA) “gel” injections, corticosteroid injections, and platelet‑rich plasma (PRP) injections. Each works differently, has a different onset and duration, and suits different patient profiles. Evidence‑based care means matching the right injection to the right person, using precise technique, and pairing treatment with a structured rehabilitation plan.
Important clinic note: Our clinic is one of the few in Singapore where you can use MediSave or your insurance to claim for knee joint injections, subject to eligibility, prevailing regulations, and your policy terms. We confirm claimability during your consultation and provide any documentation needed for pre‑authorisation or claims submission.
What are knee injections?
Knee injections deliver medication or biologic agents directly into the joint space to address pain drivers such as inflammation, synovial friction, and degenerative wear. By placing treatment where it is needed most, injections can make walking, stairs, work, and sport more manageable. They are typically considered after exercise therapy, activity modification, weight optimisation, and simple analgesics have not provided sufficient relief, or when these measures need a short‑term boost to work better.
Types of knee injections in Singapore (and how they differ)
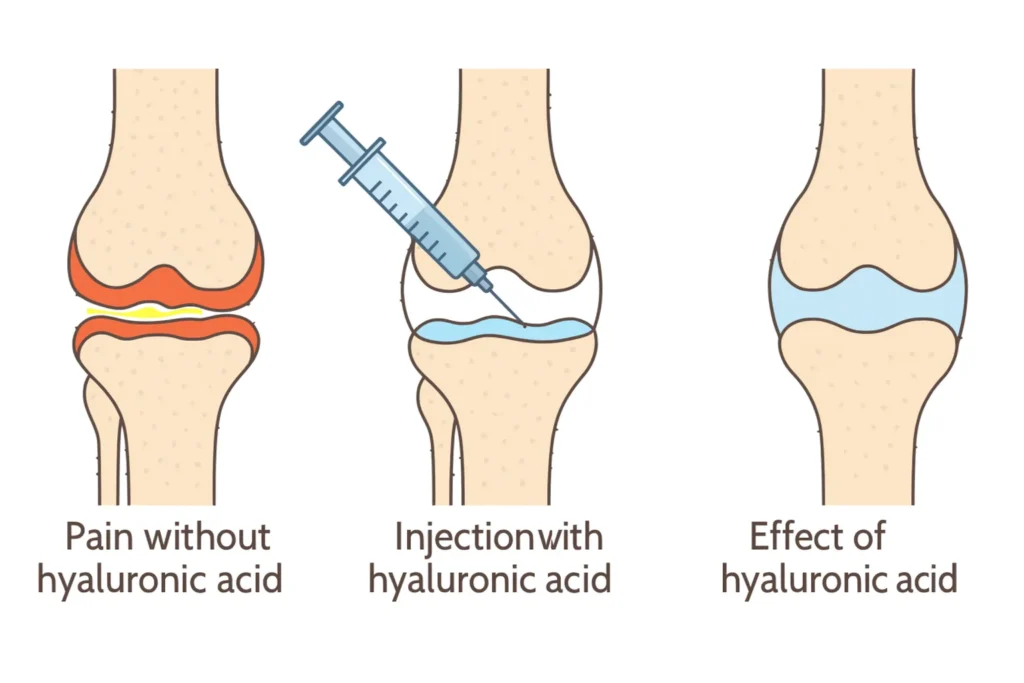
HA — “viscosupplementation” or “knee gel injections”
Hyaluronic acid is a gel‑like molecule that naturally lubricates healthy joints. In osteoarthritis, joint fluid can lose viscosity and shock‑absorbing function. HA injections supplement lubrication, reduce friction, and can ease pain. Relief usually builds over weeks rather than days and, in responders, can last several months. Products differ by molecular weight, cross‑linking, and whether they are given as a single injection or a short series.

Corticosteroid (“steroid”) injections
Corticosteroids target synovial inflammation. They are often used during flares with swelling and warmth, or when quick relief is needed to restart physiotherapy. Onset is generally fast, often within days, while duration is shorter, typically weeks to a few months. Most clinicians space steroid injections and avoid using them too frequently in the same joint.
Platelet‑rich plasma Knee Injections
PRP is prepared from your own blood and contains a higher concentration of platelets that release growth factors. The aim is to modulate inflammation and support tissue healing. Protocols vary, and so do results. Some studies report meaningful symptom improvement for months, while others show more modest benefit. PRP knee injections can be considered by patients who prefer a biologic option and understand the heterogeneity of the evidence.
Who is a candidate (and who may not be)?
You may be a good candidate if you have:
- Mild‑to‑moderate knee osteoarthritis with pain that limits walking, stairs, work, or sport.
- Persistent symptoms despite exercise therapy, load management, and simple analgesics.
- Contraindications or intolerance to certain oral medications.
- A desire to delay surgery while maintaining function through a structured rehabilitation plan.
You may not be a good candidate if you have:
- Advanced, multi‑compartment osteoarthritis with major deformity and unremitting night pain.
- An active infection or skin disease near the injection site.
- A known allergy to specific injection components.
- Medical issues that significantly increase procedural risk without commensurate benefit.
An orthopaedic assessment considers your osteoarthritis grade (for example, Kellgren‑Lawrence), limb alignment, body mass index, activity level, flare pattern, metabolic factors such as diabetes, and prior responses to treatment. This helps determine if an injection is appropriate, which option is the best fit, and when it should be performed.
The evidence at a glance (why guidelines sometimes disagree)
Different expert bodies weigh the same studies differently, so you may read conflicting advice online.
The American Academy of Orthopaedic Surgeons (AAOS, 2021) does not recommend routine use of hyaluronic acid for symptomatic knee osteoarthritis. Corticosteroid injections may provide short‑term relief for some patients.
The National Institute for Health and Care Excellence (NICE, 2022) recommends against hyaluronic acid injections and supports considering intra‑articular corticosteroids for short‑term symptom relief when other treatments are unsuitable or ineffective.
The Osteoarthritis Research Society International (OARSI, 2019) takes a patient‑profile dependent stance and allows a conditional role for HA in selected individuals, emphasising shared decision‑making.
These positions reflect mixed evidence, cost‑effectiveness considerations, and the reality that knee osteoarthritis is not a single disease but a set of phenotypes. In practice, HA can be reasonable for selected patients who value its local action and accept that responses vary. Steroid is used for flares and short‑term goals. PRP remains a consideration in clinics that offer it, with transparent counselling about protocol differences and evidence variability.
Why technique matters: ultrasound‑guided vs landmark injections
Accuracy matters in knee joint injections. Ultrasound guidance allows your clinician to visualise the needle path and confirm intra‑articular placement in real time. Higher accuracy is associated with fewer failed attempts and, in some cohorts, better patient‑reported outcomes. In practical terms, better accuracy means a higher likelihood that the medication is delivered precisely into the joint space. Our clinic uses ultrasound guidance as standard for knee injections because precision supports both safety and outcomes.
HA brands you will hear in Singapore (and how to choose among them)
Patients frequently ask about Monovisc, Orthovisc, Cingal, and Synvisc. These are all HA‑based products, but they differ in ways that matter to your experience.
- Monovisc® is a single‑injection hyaluronic acid viscosupplement. It is designed for convenience and suits people who prefer one visit with a gradual, multi‑month symptom curve in responders.
- Orthovisc® is commonly administered as a series of three or four weekly injections. Some patients like the staged approach, and some clinicians prefer to distribute dosing over several weeks.
- Cingal® combines HA with a corticosteroid in one syringe. The rationale is faster early relief from the steroid and sustained lubrication from the HA. This option is attractive if you want both quicker onset and longer‑term benefit without multiple visits.
- Synvisc®/Synvisc‑One® are other widely used hyaluronan formulations. Synvisc is often given as a three‑injection series, while Synvisc‑One is administered as a single injection.
There is no universal “best” product. The right choice depends on your symptom pattern (flare‑dominant versus steady pain), convenience preferences (single visit versus series), prior responses, budget, and medical profile. Your clinician will also consider formulation details such as molecular weight and cross‑linking, and will screen for any relevant allergy risks.
Cost, MediSave, and insurance in Singapore (and what makes our clinic different)
Patients understandably ask about cost and coverage. In Singapore, prices vary by brand, dose, whether ultrasound guidance is used, and whether your package includes reviews or physiotherapy. Many clinics state that viscosupplementation is not MediSave‑claimable.
Our clinic is different. We are one of the few clinics in Singapore where MediSave or insurance claims for knee joint injections are possible, subject to medical indication, Ministry of Health rules, and your policy’s terms and pre‑authorisation requirements. During your consultation, we provide a clear written estimate, confirm eligibility, and help with any insurer documentation so that your plan is financially predictable.
What to expect: before, during, and after your injection
Before the injection. You will have a consultation that includes history, examination, and review of existing imaging. If needed, we may order X‑rays or ultrasound to clarify severity and exclude other causes of pain. We will discuss your goals, whether an injection is appropriate, and which option best fits your situation. We will also review your medications and provide pre‑injection instructions.
During the injection. The procedure is performed in a clean outpatient setting. After skin antisepsis and local anaesthetic at the needle entry point, we use ultrasound guidance to place the medication precisely within the joint. Most injections take only minutes and are well‑tolerated.
After the injection. Mild soreness for 24 to 48 hours is common. We usually recommend avoiding high‑impact activity for a couple of days and then gradually resuming your routine. Steroid benefits tend to appear quickly. HA and PRP often build over weeks. We schedule follow‑up to track functional goals such as stair tolerance, walking time, and morning stiffness because these measures reflect meaningful progress.
Benefits and risks (clear expectations)
Potential benefits. Knee injections can reduce pain and improve function so that you can participate more fully in rehabilitation. For some patients, injections help defer surgery until it is truly necessary or until life circumstances are more favourable. HA has a low systemic side‑effect profile compared with long courses of oral analgesics. Steroid offers rapid relief during flares. PRP provides a biologic alternative for patients who prefer it and understand its variability.
Potential risks. Most side effects are minor and transient, such as brief soreness, warmth, or swelling at the injection site. Infection is rare but serious, so sterile technique and ultrasound guidance are used to minimise risk. Allergic reactions are uncommon, and allergy history is reviewed beforehand. Steroid injections can transiently raise blood sugar in people with diabetes. The most important practical risk is non‑response; some knees do not improve with injections. Careful selection and realistic goal‑setting help manage this possibility.
Alternatives and complements to injections
Exercise therapy and strength training remain core elements of osteoarthritis care. Injections often make it easier to participate consistently.
- Weight optimisation, activity pacing, and footwear or insoles can reduce symptom load with minimal downside.
- Topical NSAIDs and judicious short courses of oral analgesics can be used as part of a balanced plan.
- Bracing can help selected wear patterns by redistributing load.
- Shock‑absorbing surfaces at home or work and load management in sport prevent symptom spikes that derail progress.
When injections are not enough: thinking about surgery
When pain wakes you at night, your knee buckles or feels unstable, and function remains severely limited despite best conservative care, it is time to discuss surgical options. Depending on wear pattern and alignment, these may include unicondylar (partial) knee replacement or total knee arthroplasty. Surgical planning aims to restore alignment, joint‑line position, and balanced soft tissues. Dr Gerard Ee has co‑authored peer‑reviewed work in The Knee showing the value of computer navigation as a tool for measuring and restoring the joint line during total knee arthroplasty. That precision ethos carries into all treatment decisions in clinic.
Why choose Dr Gerard Ee’s programme?
Academic pedigree in knees
Dr Gerard Ee has co‑authored peer‑reviewed papers in respected journals, including The Knee and Knee Surgery, Sports Traumatology, Arthroscopy. His work on computer navigation for joint‑line measurement connects directly to what patients care about: alignment, balance, and functional outcomes.
Evidence‑balanced counselling
You will hear the upsides and limits of steroid, HA, and PRP, and you will understand why guidelines sometimes disagree. Your choice will match your goals, budget, and timeline.
Technique that respects accuracy
Ultrasound guidance is used routinely for knee injections because precision matters.
Financing made simpler
Unlike many clinics, MediSave or insurance claims for knee joint injections may be available at our clinic, subject to indication and policy terms. We handle the paperwork with you.
Rehab‑centric approach. We pair injections with physiotherapy and strength programming because injections work best when they enable consistent training.

Frequently asked questions
Which lasts longer — steroid, HA, or PRP?
Steroid typically offers faster onset but shorter duration, often weeks to a few months. HA and PRP may take longer to kick in but can last months in responders. The best option depends on osteoarthritis severity, inflammation levels, activity demands, and prior responses.
Is hyaluronic acid “worth it” if some guidelines recommend against it?
It can be worthwhile for selected patients who value its local action and accept that responses vary. We will help you weigh evidence, cost, and expectations so your decision is informed and comfortable.
Is ultrasound guidance really necessary?
It is not mandatory, but it improves accuracy and may improve outcomes. We use ultrasound guidance routinely to ensure precise intra‑articular delivery.
Can injections delay knee replacement?
In some people, yes—especially when injections enable consistent rehabilitation and load management. In others with advanced wear or significant deformity, injections may not provide adequate relief and surgery can be the better path.
Are knee injections safe if I have diabetes or I am on blood thinners?
Many patients with these conditions receive injections safely, but plans must be individualised. Steroid injections can transiently raise blood sugar, so we coordinate with your primary doctor when needed. For anticoagulants, we evaluate bleeding risk and adjust technique or timing accordingly.
Are hyaluronic acid injections MediSave‑claimable?
At many centres, viscosupplementation is not claimable. At our clinic, MediSave or insurance claims for knee joint injections are possible when criteria are met. We guide you through eligibility and pre‑authorisation before you proceed.
If you are considering knee injections in Singapore, book a consultation. We will confirm your diagnosis, explain the pros and cons of each option, advise on MediSave and insurance claimability, and design a plan that pairs precise injection technique with rehabilitation to help you move with confidence again.
No Comments